The Anterior Cruciate Ligament (ACL) connects the front top of the tibia (the lower leg bone) to the rear bottom of the femur (the thigh bone). Athletes are often diagnosed with this common sports knee injury.
Causes
An ACL (anterior cruciate ligament) injury can occur due to a variety of causes including:
Sports-related activities: Sudden stops, changes in direction, or jumping in sports can stress the ACL.
Direct trauma: Knee injuries from car accidents or falls can strain or tear the ACL.
Improper landing techniques: Poor form during jumping or landing on a flexed knee or with excessive force can increase ACL injury risk.
Overuse and repetitive stress: Continuous strain on the knee joint, especially in activities that stress the ACL, can make individuals more susceptible to ACL tears.
Previous injury: Individuals with a history of ACL injury are at increased risk of re-injury.
Risk factors
Several studies have shown that female athletes have a higher incidence of ACL injury than male athletes in certain sports, possibly due to pelvic or lower leg alignment. Also, engaging in sports and physical activities that involve cutting, pivoting, jumping, or sudden changes in direction can significantly increase the risk of ACL injuries. Sports such as soccer, basketball, football, skiing, and gymnastics are particularly associated with a higher incidence of ACL tears.
Symptoms
Symptoms of an ACL (anterior cruciate ligament) injury can include:
“Popping” noise and feeling of knee “giving out”: Many individuals report hearing or feeling a distinct “popping” sound or sensation at the time of injury. This can occur during a sudden change in direction, landing from a jump, or a direct impact to the knee.
Pain with swelling: After an ACL injury, the affected individual may experience pain in the knee. The pain can range from mild to severe, depending on the extent of the injury. Swelling around the knee joint is also a common symptom, often occurring within the first few hours following the injury.
Loss of full range of motion: The individual may find it difficult or impossible to fully bend or straighten the knee after an ACL injury. The range of motion is often limited due to the instability caused by the ligament damage.
Tenderness along the joint line: The area along the joint line, where the ACL is located, can become tender to touch. Pressing on or palpating this area may elicit pain or discomfort.
Difficulty and discomfort while walking: Walking can become challenging and uncomfortable following an ACL injury. The knee may feel unstable, causing the individual to have difficulty bearing weight on the affected leg. This can result in a noticeable limp or an altered gait pattern.
Diagnosis and treatment
Diagnosis usually involves a physical examination from an orthopedic surgeon, although sometimes imaging tests such as an x-ray or MRI scan help the doctor confirm diagnosis.
Nonsurgical treatment can include bracing or physical therapy, but a torn ACL will not repair itself. Surgical treatment usually involves arthroscopy, where a tiny camera is inserted in the knee through a small incision and connected to a video monitor in the operating room. Your surgeon uses the camera to repair the damaged ACL with tissue from another part of your body, typically a tendon from your knee or hamstring, or from a cadaver. There are risks and benefits to each kind of replacement tissue. ACL reconstruction is usually very successful and rehabilitation includes physical therapy. The patient may return to sports when there is no longer pain or swelling, when full knee range of motion has been achieved, and when muscle strength, endurance and functional use of the leg have been fully restored, typically 4-6 months.
Body
Shoulder impingement is also known as rotator cuff tendinitis. It occurs when the rotator cuff tendons rub against (or impinge) on the shoulder blade, which causes pain and irritation.
Causes and risk factors
This condition is common in young athletes, especially for tennis players, baseball players, and swimmers. It is also common for those with occupations that require repetitive overhead movement, such as painting or construction. Several factors can contribute to the development of shoulder impingement, including:
Repetitive overhead activities: People who engage in repetitive overhead movements or activities that involve raising the arm, such as swimming, tennis, or weightlifting, are at a higher risk of developing shoulder impingement.
Poor posture: Rounded shoulders or forward head posture can alter the alignment of the shoulder joint, increasing the likelihood of impingement.
Shoulder instability: Individuals with shoulder instability, where the shoulder joint is loose or prone to dislocation, may experience impingement due to the abnormal movement of the humeral head within the joint.
Bone abnormalities: Certain anatomical variations, such as the shape of the acromion (a bony process of the shoulder blade), can contribute to the narrowing of the subacromial space and impingement.
Aging: As we age, the structures in the shoulder can degenerate, including the tendons and bursa. This degeneration can increase the risk of impingement.
Trauma or injury: A previous shoulder injury or trauma, such as a dislocation or fracture, can lead to structural abnormalities or inflammation that predispose an individual to impingement.
These factors increase the risk of developing shoulder impingement, but they may not always directly cause the condition. A comprehensive evaluation by a healthcare professional is essential to determine the underlying causes and provide appropriate treatment.
Symptoms
Shoulder impingement can cause a range of symptoms that typically involve pain and limited range of motion in the affected shoulder. Common symptoms of shoulder impingement include:
Shoulder pain: The most common symptom of shoulder impingement is pain, which is often felt on the front or side of the shoulder. The pain may be dull and aching or sharp and intense. It can worsen with certain movements, especially when raising the arm overhead or reaching behind the back.
Painful movements: Activities that involve raising the arm or reaching across the body can trigger or worsen the pain. Pain may also be experienced during activities like lifting, throwing, or even simple tasks such as reaching for objects on high shelves.
Weakness: Shoulder impingement can cause weakness in the affected shoulder, making it difficult to perform certain movements or lift objects. Weakness may be particularly noticeable when trying to lift the arm against resistance or when performing tasks that require strength.
Limited range of motion: Impingement can restrict the normal range of motion in the shoulder joint. You may experience difficulty in fully raising the arm, rotating it, or reaching behind the back. Activities like putting on clothes, combing hair, or fastening a bra may become challenging.
Shoulder stiffness: Impingement can lead to shoulder stiffness, making it feel tight and difficult to move the joint freely. This can affect daily activities and result in decreased mobility.
Treatment
Treatment for shoulder impingement typically begins with conservative measures and may progress to surgical intervention if symptoms persist. Conservative options include rest, anti-inflammatory medications, cortisone injections, and physical therapy. Resting the shoulder helps promote healing and reduces irritation, while anti-inflammatory medications help reduce pain and inflammation. Cortisone injections deliver powerful anti-inflammatory medication directly to the joint for temporary relief. Physical therapy plays a vital role in strengthening the shoulder muscles and improving mechanics through tailored exercises and manual therapy techniques.
If conservative treatments do not provide sufficient relief, surgical intervention may be considered. Arthroscopic surgery is the most common approach, involving small incisions for the insertion of a camera and surgical instruments. The surgeon removes inflamed tissues and may trim the acromion bone to create more space in the joint. In some cases, an open surgical technique with a larger incision may be chosen to directly access the joint and address impingement or structural abnormalities. Post-surgical rehabilitation, including physical therapy, is crucial to restore strength, range of motion, and function to the shoulder joint gradually.
It’s important to consult with a healthcare professional to determine the most appropriate treatment plan for shoulder impingement based on individual factors such as symptom severity, underlying causes, and overall health.
Body
Knee replacement can help relieve knee pain and enable you to live a fuller, more active life. If you and your orthopedic surgeon have decided that you are a good candidate for a full joint replacement, you are in good company. Almost one million hip and knee replacement surgeries are performed in the United States annually, making it one of the most common orthopedic procedures performed today.
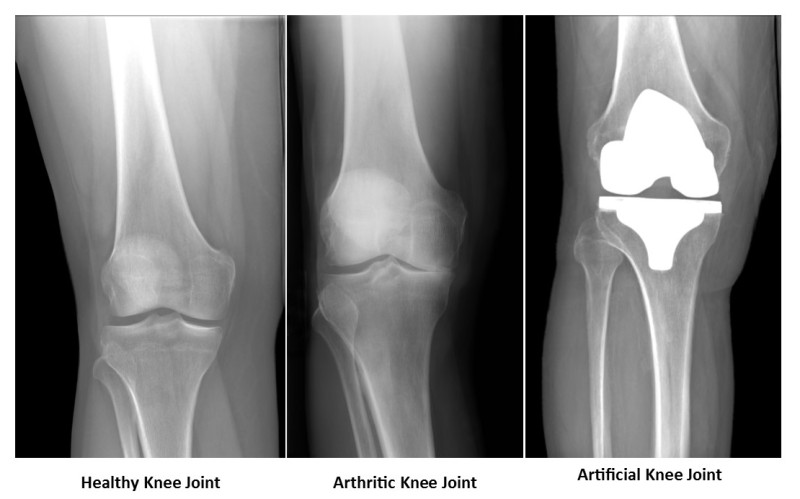
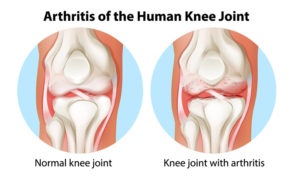
The knee functions as a hinge joint. The joint is made from the end of the thigh bone (femur), where it meets the shin bone (tibia) and the knee cap (patella). Normally, the cartilage coating over the bones makes the joint move smoothly and provides an additional shock-absorbent cushion. In an arthritic knee, the cartilage surface wears out and begins rubbing bone on bone which causes pain, stiffness, and swelling of the knee joint.
In a total knee replacement surgery, the arthritic surfaces of the knee joint are removed and new surfaces are provided with metal and poly (plastic) parts. This relieves knee pain and allows the joint to move smoothly again.
Body
The rotator cuff is a common source of pain or injury in the shoulder. It plays a role in the normal function of the shoulder by contributing to the stability of the joint. It is formed of tendons which attach to the humerus, as well as four major muscles which drape over the shoulder joint.
Causes and risk factors
A rotator cuff injury can occur due to various causes and risk factors, including:
Direct blow, fall, or sports-related injury: Traumatic events such as a direct blow to the shoulder, a fall onto an outstretched arm, or sports-related injuries can damage the rotator cuff. These injuries may result from contact sports, accidents, or sudden impacts.
Degenerative conditions, such as arthritis: Degenerative changes in the shoulder joint, commonly associated with arthritis, can contribute to a rotator cuff injury. Arthritis can lead to the wearing down of the cartilage and bones in the shoulder, making the rotator cuff more susceptible to damage.
Repetitive stress: Certain sports and activities that involve repetitive shoulder movements can increase the risk of developing a rotator cuff injury. Athletes involved in overhead sports like baseball, tennis, swimming, or weightlifting, which require frequent and forceful use of the shoulder joint, may experience repetitive stress on the rotator cuff. Over time, this can lead to inflammation, tendon degeneration, and eventual injury.
Bone spurs: Bone spurs, also known as osteophytes, are bony projections that can develop on the edges of bones. In the case of the shoulder joint, bone spurs can form on the acromion (a part of the shoulder blade) or other structures, potentially impinging on the rotator cuff tendons. The presence of bone spurs can increase the risk of rotator cuff tears by causing friction, irritation, and impingement on the tendons during shoulder movements.
Symptoms
A rotator cuff injury can present with various symptoms, including:
Shoulder pain: One of the primary symptoms of a rotator cuff injury is shoulder pain. This pain can be constant or may occur when you are at rest, especially during nighttime when lying on the affected shoulder. The pain is often localized to the front or outer part of the shoulder and can radiate down the arm.
Pain or weakness when lifting or lowering your arm: Another common symptom is experiencing pain or weakness when lifting or lowering your arm. Activities such as reaching overhead, carrying heavy objects, or performing certain movements may exacerbate the pain. You may also notice a decrease in strength and difficulty in performing tasks that require arm movements, especially those involving lifting or reaching.
Limited range of motion: A rotator cuff injury can lead to a decrease in your shoulder’s range of motion. You may find it challenging to move your arm fully or lift it above a certain point. Activities like combing your hair, reaching behind your back, or putting on clothes may become difficult due to this restricted mobility.
Clicking or popping: In some cases, individuals with a rotator cuff injury may experience clicking or popping sensations in the shoulder joint during certain movements. These sounds can indicate structural abnormalities, such as a tear or impingement within the rotator cuff.
Diagnosis and treatment
Your doctor will evaluate your shoulder by conducting a physical examination. They will assess your range of motion, strength, and areas of tenderness or pain. To confirm the diagnosis and assess the extent of the injury, imaging tests may be ordered. These can include X-rays to rule out other conditions and provide information about the bone structures, as well as MRI (Magnetic Resonance Imaging) or ultrasound to visualize the soft tissues, including the rotator cuff tendons.
Non-surgical treatments include anti-inflammatory medications, rest, ice, corticosteroid injections, and/or physical therapy. Surgical repair may be an option, depending on the severity of the injury. Your orthopedic surgeon may recommend surgery to repair a torn rotator cuff if your symptoms don’t go away after conservative treatment, you have a large tear (more than 3cm), or if it was caused by a recent trauma.
Recovery after surgery
Most patients will go home the same day of surgery. After your surgery, your care team will put the brace on your arm before you wake up. Your doctor will let you know when it’s okay to take the brace off. You’ll need to remove it for showering and dressing.
This video provides detailed instructions for using your shoulder sling after surgery.
Recovery timeline
First week: Immediate post-surgery
Rest: Keep your shoulder in a sling. Rest and manage pain with medications and ice.
Wound Care: Follow instructions for keeping the surgical site clean and dry.
Weeks 2-4: Early rehabilitation
Healing: Continue using the sling. Begin gentle passive range-of-motion exercises as advised by your physical therapist.
Follow-Up: Attend appointments to monitor progress and adjust treatment.
Weeks 5-8: Progressive rehabilitation
Physical Therapy: Start more active exercises to restore range of motion and strength. Gradually resume light activities.
Sling: Your surgeon will advise when to stop using the sling.
Months 2-4: Strengthening and Functional Recovery
Advanced Therapy: Focus on strengthening exercises and return to normal activities. Continue supervised physical therapy.
Activity: Gradually resume sports or heavier lifting with your surgeon’s approval.
Months 4-6: Full Recovery
Normal Activities: Most normal activities can be resumed. Maintain a regular exercise routine to support shoulder health.
Final Assessment: Confirm recovery status with your healthcare provider.
Beyond 6 Months: Long-Term Maintenance
Preventive Care: Continue shoulder exercises and good posture practices. Schedule regular check-ups to monitor long-term health.
This timeline provides a general guide; individual recovery may vary based on specific circumstances. Always follow your healthcare provider’s recommendations.
Body
The spine is made up of a stack of vertebrae that normally appear in a fairly straight line. When scoliosis is present, the spine has a sideways curve that can appear as an S or C. The condition is usually present in children and adolescents. Most cases of scoliosis are mild, and a small curve will likely not cause major problems. More severe cases of scoliosis can have more debilitating effects.
Causes and risk factors
There are several types of scoliosis that are caused by different things.
Idiopathic scoliosis causes 80-85% of scoliosis cases and the cause is unknown. It tends to run in families, but there is nothing that can be done to prevent the condition. Signs and symptoms usually present themselves prior to puberty.
Congenital scoliosis begins to affect the spine before birth. The vertebrae do not form completely or separate properly. Because abnormalities are present at birth, congenital scoliosis is usually diagnosed at a younger age than idiopathic scoliosis.
Neuromuscular scoliosis occurs when another condition that affects the nerves and muscles leads to scoliosis. This is commonly due to muscle imbalance and/or weakness. Common neuromuscular conditions that may lead to scoliosis include cerebral palsy, muscular dystrophy, or a spinal cord injury.
Symptoms
Uneven shoulders
One shoulder blade that is more prominent than the other
One or both hips appear raised or unusually high
Uneven waist
Head does not appear centered with the rest of the body
Asymmetric ribcage
Treatment
Most children with mild scoliosis will not require any treatment. Your doctor will likely monitor your child closely every four to six months to make sure there are no changes in the curvature of the spine. If your doctor is concerned that the curve may worsen over time, they may recommend bracing. A brace can help prevent the curve from getting worse as your child continues to grow.
More severe cases of scoliosis may require surgery to reduce the severity of the curve and prevent it from getting any worse.
Osteoarthritis usually develops after years of use. It is common in the knees because the knees bear the weight of the body. Over time, the cartilage in the knee wears down and stops protecting the ends of bones in the joint.
Causes and risk factors
Wear and tear of aging
Traumatic injury to the joint
Developmental dysplasia
Inflammatory arthritis
Osteonecrosis
Infection
Metabolic disorders
Hemoglobinopathies and other blood disorders
Autoimmune disorders
Obesity
Symptoms
Pain, swelling, and stiffness
The knee may lock or buckle when walking
Trouble bending or straightening the knee
Standing or walking for long periods may worsen pain
Diagnosis and treatment
Nonoperative treatment options include injections, physical therapy, taking anti-inflammatories, activity modification, weight loss, bracing, and using a cane/walker. If these are not helpful, an orthopedic surgeon may recommend surgery such as total knee replacement (knee arthroplasty) to relieve pain and preserve mobility.
Body
Vertical talus is a congenital foot disorder, meaning it is present at the time of birth. It appears as an extreme case of flatfoot and may affect one or both feet. Though vertical talus is not painful for a newborn or young child, it can lead to serious problems and discomfort later in life. The talus is a small bone that connects the foot and leg, and sits between the heel bone (calcaneus) and the two bones of the lower leg (tibia and fibula). The tibia and fibula work with the talus to form the ankle joint. In vertical talus, the talus has formed in the wrong position and other foot bones have formed on top of the talus. As a result, the foot typically points up and the bottom of the foot is stiff with no arch.
Causes and risk factors
The exact cause of vertical talus is not known, though it is often associated with the following conditions:
Arthrogryposis
Spina bifida
Neurofibromatosis
Other neuromuscular diseases
Symptoms
Vertical talus is a foot disorder that’s usually diagnosed at birth, or before, if it is visible on an ultrasound.
Treatment
Vertical talus will not resolve itself and requires medical attention. It is important for vertical talus to be treated early before the deformity has time to progress. If your child learns to walk with an abnormal foot, painful problems can develop. Nonsurgical treatment options for vertical talus include:
Stretching or casting
Physical therapy
If the deformity does not correct with conservative treatment, surgery is usually required. Your pediatric orthopedic surgeon will put the bones in the correct position and fix any issues with the tendons and ligaments supporting the bones. A brace or special shoe may be recommended to prevent the deformity from returning. With treatment, you can expect your child to have a stable and functional foot.
Before becoming the St. Charles Center for Orthopedics & Neurosurgery, The Center had a long history in Central Oregon.
The Center got their start in 1958 when the Bend Orthopedic & Fracture was founded. Then, in 1979, the Bend Neurosurgical Group was founded. In 1999, the two groups merged to form The Orthopedic & Neurosurgical Center of the Cascades.
The arch of the foot helps to support us when we stand up or walk. Most children are born with very little arch in the feet. As they grow, develop, and begin to walk, the soft tissues along the bottom of the feet tighten and begin to shape into an arch. When the arch in the foot is not present, the condition is known as flatfoot. There are two types of flatfoot: flexible flatfoot and rigid flatfoot. In flexible flatfoot, the arch is present when the foot is not bearing any weight, but disappears when standing or walking. In rigid flatfoot, the arch is never present, whether bearing weight or not.
Causes and risk factors
Flatfoot is caused by abnormal foot development and can be hereditary.
Symptoms
Some children with flatfoot may have no symptoms, and children with flexible flatfoot often outgrow the condition eventually. Flexible flatfoot is typically not painful, while rigid flatfoot may cause pain during regular activities. See your pediatric orthopedic surgeon if your child experiences:
Recurring foot pain, particularly in the heel or arch area
Pain that worsens with activity
Swelling along the inside of the foot
Treatment
Children with flexible flatfoot usually outgrow the condition as their foot ligaments continue to develop. Treatment for flatfoot is only necessary if your child begins to experience pain or discomfort from the condition. Nonsurgical treatment options include:
Occasionally, flexible flatfoot can become rigid instead of correcting with growth. These cases may require surgical treatment to repair tendons or ligaments, or correct bone abnormalities.
Body
Cavus foot is a condition in which the foot develops an unusually high arch. Because of the high arch, an excessive amount of pressure is placed on different parts of the foot while standing or walking. This condition usually develops slowly during the adolescent years, and may be present in one or both feet.
Causes and risk factors
Most commonly, children develop cavus foot due to a nerve or muscle condition such as cerebral palsy, spina bifida, muscular dystrophy, or clubfoot. These conditions cause some muscles to be weaker than others, and unbalanced muscles work unevenly. Cavus foot may also occur due to an injury to the nerves in the leg or spinal cord. It may also be caused by an inherited structural abnormality.
Symptoms
The most obvious symptom of cavus foot is a very high arch in the foot, even when standing. Children may also experience the following symptoms:
Calluses or blisters on the side, heel, or balls of the feet
Bent toes (hammertoes) or flexed toes (claw toes)
Pain when walking or standing
Unstable feet due to the heel tilting inward, which can lead to frequent ankle sprains
Treatment
The first step of treating cavus foot is to determine the underlying cause. If linked to a neurological or muscular condition, it will likely worsen over time. In the very early stages or with mild cases of cavus foot, surgery may not be necessary. Non-surgical treatment options include:
Shoe inserts, such as arch supports
Shoe modifications
Bracing
If conservative treatment does not relieve pain and improve stability, your pediatric orthopedic surgeon may recommend surgery.