When a piece of hardware – like a screw – needs to be inserted into a patient’s spine, it’s important that it is placed in precisely the right spot.
“The margin for error is very, very small when inserting instrumentation into the spine. One to two millimeters can make a huge difference as to where you put a screw into the spine,” said neurosurgeon Dr. Raymond Tien.
Now, thanks to donors to St. Charles Foundation, spinal surgeons in Central Oregon are the first in the state to have access to a new, state-of-the-art spinal navigation system to help ensure that spinal surgeries performed at St. Charles are incredibly accurate. The SeaSpine 7D spine navigation system arrived last fall and it allows surgeons to see the spine in three dimensions while inserting a piece of hardware.
Tien recently used the system to place hardware in the spine of a patient.
“The procedure went perfectly and faster than it would have gone previously. It’s eye opening how accurate this system is and how easy it is to use,” said Tien.
Patients may need this kind of procedure due to a degenerative or congenital condition or medical trauma, like a fall or car crash. When placed correctly, hardware can help stabilize an unstable spine.
For the past 20 years, surgeons performed spinal surgeries using an X-ray unit in the Operating Room to help them visualize the anatomy. Tien says surgeons took many X-rays of the spine to create as complete a picture as possible. However, he says, the two-dimensional images are not as accurate as 3D images – and the process exposed everyone in the room to a lot of radiation.
With the new system, patients get a high-resolution CT scan prior to surgery. That scan is uploaded to the computer as a reference. Surgeons then place a marker on the patient’s spine that a camera can see. The navigation system has an array of lasers and light-emitting diodes that take a flash photo of the marker exposed in the spine. With those images, surgeons then have an accurate 3D model of a patient’s spine.
“We can see directly on the computer where we are touching and see in very high fidelity where we are inserting the hardware and make adjustments on the fly,” said Tien. “This tool provides us an incredible level of accuracy and precision.”
St. Charles Foundation Executive Director Jenny O’Bryan says this piece of equipment is the largest investment the organization made in 2024 – spending nearly $700,000 to bring the SeaSpine 7D spinal navigation system to Central Oregon.
“Our donors want to ensure that Central Oregonians are receiving the best care possible from the best providers, utilizing the best equipment available. If you or your loved ones need spinal surgery, you want to know that your surgeons have the best equipment on hand. Thanks to our donors, that’s the case,” said O’Bryan.
In addition to its precision, Tien says the new tool also helps save time for patients. He also believes it will allow for surgeons to take on more complex cases.
“There is a real tangible value in the level of patient care that we can provide now that we weren’t able to prior to this,” said Tien. “Without a doubt, we are very grateful for what the donors to the Foundation have been able to do for the hospital and for the community.”
Our one-on-one sports nutrition sessions are designed to help athletes meet their performance goals by creating customized fueling strategies that align with their training demands, recovery needs and lifestyle.
What to Expect
Initial Session: Setting the Foundation
In our first session, we’ll dive deep into your current training regimen and performance goals. Together, we will:
Identify potential gaps in your fueling strategy
Explore your current eating and exercise habits
Review lab work and recommend any necessary micronutrient support
Discuss financial or lifestyle factors that may impact nutrition choices
Provide foundational sports nutrition education
Customize your nutrition plan based on your sport, goals and daily routine
Encourage energy, diet and training tracking to assess patterns and make data-informed decisions at future sessions
Follow-Up Sessions: Continued Support and Optimization
Ongoing sessions are tailored to support your evolving needs and keep you on track. These may include:
Reviewing your food and training logs
Assessing progress and outcomes from previous recommendations
Identifying and addressing barriers to success
Offering targeted nutrition education
Refining goals and updating your fueling plan as your training progresses
Whether you're aiming for peak performance, improved recovery or simply want to feel your best during training and in daily life, we’ll work together to build a plan that fits your unique needs.
St. Charles Health System announced today recipients of a variety of Community Benefit grants, awarding more than $100,000 to 31 local organizations in Central Oregon. The grants were awarded to provide basic needs, sponsor local events and as part of St. Charles’ Priority Grant to increase a sense of belonging and reduce loneliness and isolation.
From funding food boxes in schools to community activities at a local senior center, the grants will help communities across Central Oregon with a wide range of needs.
Hearts Unknown Education, a local nonprofit that supports art and music for at-risk youth, received $7,500 to expand its programming. The local nonprofit offers a safe, welcoming space for students to create art and music, while also providing support for positive mental health.
“Many kids need a place to feel like they can be themselves and feel free to express themselves through art and music in an environment where they are appreciated for being themselves,” said Nicola Carpinelli, director of HUE, which serves more than 100 youth every week through a variety of programs. “This funding is going to help us maintain and expand offerings and we are grateful for the support from St. Charles.”
Learn more about St. Charles Community Benefit program on our website.
Physician Associate Mandi Bryson went into family care medicine because she wanted to help people. “I love building relationships with patients,” said Bryson, who works at St. Charles' Bend East Family Care Clinic.
But in recent years, Bryson found herself tied to her computer more and more, due to increasing documentation requirements, inbox messages and phone calls to return. “There was a mental burden of all the stuff that you have to do that’s not taking care of the patient in front of you,” said Bryson. She found herself leaving the clinic about 6 p.m. and then spending an additional hour or two at home every night completing required documentation on the computer.
Last spring, the stress became so overwhelming that Bryson considered leaving the profession all together.
“I was desperate. The demands were so heavy, I was looking for other jobs. I knew I couldn’t continue to do this to myself. What was a life-giving job had become too much. I thought, ‘Either I get something that helps me, or I have to leave this work that I love,’” she said.
Bryson got help with the burdens of technology from an unlikely source - new artificial intelligence software called DAX. Not only has this technology cut charting time significantly, but it has also allowed Bryson and other physicians to better connect with patients during exams. That’s because the technology completes the documentation, allowing providers to focus all their attention on their patients.
“This has been a game changer. I’ve stopped applying to different jobs,” said Bryson, who says she is now leaving work by 5:30 p.m. with notes done and an empty inbox. “I love my work. There are still challenging aspects, but documentation isn’t one of them. I can focus more on the parts that bring me joy.”
She is one of approximately 55 primary care providers at St. Charles now using DAX and there are plans to bring the service to other clinical areas.
“DAX allows providers to get to do what called them to medicine in the first place – caring for patients,” said Dr. Matt Clausen, ambulatory chief medical informatics officer, who led the effort to bring DAX to St. Charles.
DAX is more than a transcription service; it uses artificial intelligence to summarize and provide accurate notation within a patient’s electronic health record. Physicians using DAX first get permission from patients to use the service – then, they pull the app up on their phone as they walk into a patient’s room. The provider conducts the exam with the patient as usual – but there is no need to take notes or sit by a computer. Instead, the physician can focus entirely on the patient while DAX listens in the background and fills in the patient’s chart. Providers review the notes to ensure accuracy, but it significantly cuts down the time spent charting.
Clausen says burnout among physicians has increased in the past few years and he believes that is directly linked to the demands of documentation. This AI tool was brought in specifically to help with burnout and the results have been overwhelmingly positive.
Before using DAX, 47% of St. Charles primary care providers said they were “definitely burning out” and experienced more than one symptom of burnout. After implementing the DAX program, that dropped to just 7 percent of providers. Physicians using the technology also reported higher job satisfaction (88%), that they are more likely to continue practicing medicine (75%), that they have better documentation quality (88%) and better work-life balance (75%).
“We are early adopters for this technology and we are already seeing it help us with recruitment and retention,” said Clausen.
But perhaps the most significant aspect of this technology is its impact on patients. Eighty-nine percent of patients said that their provider was more focused during their visit when they used DAX and 100% said their provider spent less time on the computer.
Dr. Nathan Thompson, a family care physician in Redmond, says doctors have a choice: Do I chart in the room and look at my computer or do I give my attention to the patient and try to remember everything they are saying to document later? “It’s a horrible tension,” he said.
Now, with DAX, that tension is gone.
He said documentation used to take him up to 20 minutes per patient before DAX. Now it’s down to minutes of review. For Thompson that means he now has time to volunteer coaching soccer at a local high school and he is more able to be present mentally, physically and emotionally to his family.
Thompson worried that some of his patients might be skeptical of the technology. “I worried a lot of people would not go for it, but it’s been the complete opposite. I am very grateful to our community for accepting it. I want them to know this is only something we use to be more present as humans. It’s allowing us to be more human in the room.”
Bryson agrees that her patients have also been very supportive of the technology.
“I’m hearing from patients, ‘you were really listening; it felt like you weren’t rushed; I’ve never had an appointment like this.’ It’s so nice to not have a computer between me and them,” she said. “St. Charles really offered something that helped me where I needed it most. Day-in and day-out, this is making a difference and I am very grateful for that.”
As a physician and as a parent, I’ve never seen a case of measles. I’m not alone. The World Health Organization declared measles eliminated in the United States in 2000, thanks largely to an extremely effective vaccination program.
Because of the Centers for Disease Control’s recommended childhood immunization schedule, measles has been an afterthought for decades in America — if families thought about it at all. For many, receiving the MMR vaccine, which stands for measles, mumps and rubella, has been as routine as getting dressed in the morning and brushing teeth at night.
However, measles remains a serious disease: Airborne and extremely infectious, it can cause severe illness, complications and even death. Before there was a widely available vaccine, an estimated 48,000 people were hospitalized and 400 to 500 people died of measles in the U.S. each year.
Because it is so contagious, measles is a significant community health problem, and I firmly believe community challenges require collective solutions. With that in mind, I hope you’ll watch this video:
Our Central Oregon health care community is small, but strong. Our providers often work across organizations on important issues that impact us all. A handful of local pediatricians meet regularly to discuss emerging public health concerns for our kids. When Dr. Suzanne Mendez, a pediatric hospitalist at St. Charles, said this group was concerned about measles and wanted to work together on messaging that would encourage curiosity and conversation between parents and providers, we jumped at the chance to help.
I want to personally thank Dr. Julie Ansbaugh of Central Oregon Pediatric Associates, Dr. Michelle Mills of Summit Health and Pediatric Nurse Practitioner Ellie Millan of Mosaic Community Health for joining Mendez and her fellow St. Charles physician, Dr. Carey Allen, in the video. And I want to thank COPA, Summit and Mosaic for their vital partnership as we all work together to ensure Central Oregon is a safe and healthy place to live.
Community challenges require collective solutions. Here it is in action.
Just one day old, Gracie Abbott was swaddled and cozy, taking turns snuggling in the arms of her dad, Brennan, and her mom, Teagan, in a private room in the Family Birthing Center at St. Charles Bend. These tender early moments were particularly sweet for the Abbotts, as Gracie came close to spending her first days of life in the hospital’s Neonatal Intensive Care Unit.
When Gracie was born, she had fluid in her lungs, struggled to breathe and her oxygen level was low. But thanks to a newly implemented treatment called Interpulmonary Percussive Ventilation (IPV), respiratory therapists were able to remove the fluid and Gracie was able to safely stay with her parents.
“Without that machine Gracie would’ve been in the NICU. It was pretty scary; it felt like we almost lost her,” said Brennan Abbott, a Prineville resident.
Gracie is one of 116 infants who received IPV therapy since the treatment was implemented at St. Charles in March of 2024. The treatment is now available for infants born in Bend and Madras. Of those 116, 60% (70 infants) were able to stay with their parents and avoided the NICU.
“We see this as a tremendous success,” said St. Charles neonatologist Dr. Sue Ann Smith. “When infants are able to stay with their mothers, there are so many benefits – I call it the ABCs. It helps attachment, breastfeeding and it helps keep costs down for families.”
It also keeps those NICU beds open for infants who are in greater need.
How IPV works
Blake Andrews, manager of respiratory therapy at St. Charles, explains that with IPV, a mask is placed on the infant and then a pulsating airflow is pushed into the lungs. These little jets of air help move fluid out of the airways.
“The small bursts of air get around and behind the fluid trapped in the lungs, forcing those secretions out,” said Andrews. “It’s a pretty short intervention for a pretty big outcome.”
IPV was already used with adult populations, but was rarely used on infants, explained Smith. After attending a training by a NICU doctor from Legacy Salmon Creek hospital, Smith thought it was worth bringing to St. Charles.
Smith says infants often get fluid in their lungs, as the womb is a fluid-filled environment. This is especially common with babies born via C-section, as the fluid is often pushed out of the lungs in the birth canal.
“Sometimes babies have trouble making the transition and retain fetal lung fluid or meconium,” said Smith. If a baby is struggling with fluid in the lungs, the first step is to use a CPAP machine, a device that uses mild air pressure and is commonly used to treat sleep apnea.
“We need to get the air in there to keep the lungs open between breaths,” said Smith.
If after 20 minutes the baby is still in distress, they used to be sent to the NICU, where they receive more intensive care and treatment by specialized caregivers. But now, respiratory therapists can use the IPV treatment. The treatment is used for 10 minutes and then if there’s no positive change, babies are moved to the NICU.
The therapy is also available at the Family Birthing Center at St. Charles Madras, which allows infants to stay in Madras rather than having to transfer to St. Charles Bend for the NICU.
“We really want our babies to get to stay with their mothers, so this is really exciting,” said Smith.
And for the Abbott family, keeping Gracie close by during her first few days of life meant the world.
“I wouldn’t have wanted to leave her. I’m so glad we got to stay together,” said Teagan Abbott.
At St. Charles, we provide specialized ambulatory pharmacy services designed to support patients with complex medication needs. Our pharmacists work closely with your care team at our St. Charles Family Care clinics to ensure safe, effective and convenient medication management—all in an outpatient setting.
Our services
Personalized consultations to optimize medication effectiveness and minimize side effects.
Support for conditions like diabetes, hypertension, heart disease and more.
Access to high-cost, high-touch medications with expert guidance.
Convenient vaccinations and health screenings.
Help navigating prescription costs and coverage.
Our experienced team provides one-on-one support, right at the clinic, to answer your questions and manage your medications. We work seamlessly with your provider to ensure continuity of care. Our goal is to improve your health while making medication management easier.
Body
Susan A. Ellings Rehabilitation Unit
Lives are changed for the better every day inside St. Charles’ inpatient rehabilitation unit, where patients recover from traumatic injuries and serious illnesses. This is a place where every step forward is a triumph as patients and families heal together.
But the current facility is outdated and too small to meet the needs of all those who could benefit from it. Thanks to the generosity of our community - including donors from our annual Saints Gala and individual contributions - we are well on our way to building a new, state-of-the-art, inpatient rehabilitation unit. The Susan A. Ellings Rehabilitation Unit, named by an anonymous donor in memory of a family friend who passed away in 2014, is set to begin construction in 2026. Susan's daughter, Julie Cox, a nurse who works at St. Charles said, “It's a true honor to see that my mom's legacy will live on through the walls of St. Charles and we are so grateful for the donation. She was such a treasure to this earth. I hope that her love for life and radiant joy serve as a beacon of positivity for those who need it and is felt by all who enter the unit."
The current unit supports more than 350 patients every year and those patients experience tremendous success, with about 97% of them discharged home without readmission. But the demand is far higher than what the current unit can provide – with hundreds transferred to other programs outside of the region due to lack of space each year.
That’s why St. Charles is setting out to build a new, state-of-the-art, 23-bed unit. The new space will be designed with our patients, their families and our caregivers in mind to ensure we can care for our community now and into the future.
The new unit will include larger patient rooms to accommodate families and space for world-class services and new technology that will help patients re-learn activities like walking on the trails system in Central Oregon or cooking meals for themselves in an ADA accessible kitchen.
Patients spend an average of 12-14 days particpating in occupational therapy, physical therapy, speech therapy and orthotics appointments for 3 hours/day at least 5 days/week.
This spring more than 2,000 third graders throughout Central Oregon will learn about brain injury prevention and helmet safety through the Train Your Brain program taught by local athletic trainers, now part of St. Charles Health System. This program, formerly led by The Center Foundation, provides interactive assemblies and free multi-sport helmets to local elementary students.
“St. Charles is proud to continue this injury prevention program and to continue providing athletic trainers at eight local high schools, helping to ensure the safety and education of students in Central Oregon,” said Christy McLeod, Senior Vice President of Specialty Service Lines for St. Charles.
For 15 years, the Train Your Brain program has distributed more than 1,000 free helmets for local students every year, ensuring kids have proper head protection for activities such as bicycling, skateboarding, rollerblading and scooter riding. The 2025 program begins in April, just in time to prepare students for a safe and active summer.
The presentations include interactive demonstrations on injury prevention, helmet safety, proper fitting and care. A highlight of the assembly is the melon drop, which emphasizes the importance of wearing a helmet. Following the presentation, St. Charles caregivers and volunteers will properly fit free helmets for every student who needs one.
“Helmet safety is a simple yet crucial way to prevent serious head injuries in children,” said Stuart Schmidt, Athletic Training Program Manager at St. Charles. “Through the Train Your Brain program, we aim to instill lifelong safety habits in young students, empowering them to protect their brains while having fun. We also want to thank our school districts for recognizing the significance of this safety initiative and to our partners for making it possible to provide free helmets to every third grader in Central Oregon who needs one.”
To learn more about Train Your Brain and our athletic trainers, visit our webpage.
Body
Joint replacement can help relieve pain and enable you to live a fuller, more active life. If you and your orthopedic surgeon have decided that you are a good candidate for shoulder joint replacement, you are in good company. Over 50,000 people in the U.S. have shoulder replacement surgery each year.
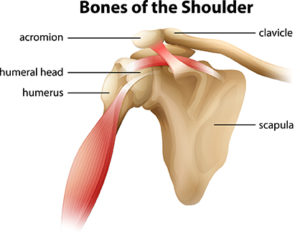
Shoulder anatomy
The shoulder joint is described as a ball and socket joint, which allows the shoulder to provide the wide range of motion required to perform many athletic activities, such as throwing, swimming, serving a tennis ball, and functional movement in many directions.
The “ball” component is made up of the head of the upper arm bone (humerus). The “socket” component, called the glenoid, is made up of the outer portion of the shoulder blade (scapula). The third bone is the collarbone (clavicle). The labrum is a rim of cartilage on the socket that helps stabilize the joint.
The stability of the shoulder joint mainly depends on the capsule, a strong envelope tissue surrounding the joint, ligaments connecting bones in the shoulder joint, tendons that attach muscles to bones, and the muscles themselves which initiate and control the position and activity of the joint. Also contributing to stability of the shoulder is the rotator cuff. The cuff formed of tendons attaches to the humerus and their four major muscles, which drape over the shoulder joint. The large muscles, which attach to the shoulder blade play a significant role in the normal function of the shoulder.
Causes and risk factors
Shoulder injuries Shoulder injuries can result from genetic factors, from overuse activities, or from a single traumatic injury. Many repetitive sporting activities that use the arm overhead, such as tennis, swimming, and baseball can result in injury to the capsule, ligaments, and muscles that surround the shoulder joint. Lifting weights too frequently or incorrectly can also lead to a shoulder injury. Immediate effects of these injuries can lead to pain, swelling, and instability of the shoulder.
Depending on the severity of the injury, the function of the injured arm can often be greatly compromised. Unfortunately, some structures of the shoulder joint do not readily heal themselves. Even with treatment, such as physical therapy, some of the symptoms or limitations may remain. Therefore, without surgical intervention, many individuals are unable to participate in their desired sports or functional activities at the pre-injury level.
Osteoarthritis This is an age-related “wear and tear” type of arthritis and a common reason that people have shoulder replacement surgery. The cartilage that cushions the bones wears away and the bones then rub against one another. Over time, the shoulder joint slowly becomes stiff and painful. In order to improve the function of the shoulder and restore motion, replacing the surfaces of the shoulder joint can be the most effective treatment to improve function and relieve pain. This can be accomplished by performing a shoulder replacement, which is also known as shoulder arthroplasty.
Surgery
The most common types of surgery are total shoulder replacement and reverse total shoulder replacement. In general, total shoulder replacement consists of putting new surfaces on the socket and humeral head. Reverse total shoulder replacement also allows for replacement of both surfaces, but does not rely on a functioning rotator cuff for motion or stability of the joint replacement. The decision to have shoulder replacement surgery, and which type, should be a collaborative one between you, your family, your primary care physician, and your orthopedic surgeon.
After surgery
Most patients are discharged home on the day of surgery unless medical issues dictate otherwise. You will be instructed how to put on and take off the sling or shoulder immobilizer and when to use it. Watch this video to learn more:
Cryotherapy, the use of cold to treat your shoulder surgery, is important to help decrease pain and reduce swelling and inflammation. You will be provided with a cold therapy unit to take home with you. Begin using it as soon as possible after you arrive home and continue using it for at least 5-7 days, during the day and night.
Your care team will provide you with prescriptions for pain medication, let you know how long to keep the dressing on, and detailed information on what to do after surgery for optimal recovery.
Recovery timeline
While not true for all patients, many will follow a similar plan during their recovery from surgery. In order to give you a sense of what is common following many shoulder surgeries we have outlined a normal post-operative timeline.
Weeks 1-2
You will work to get your pain under control, minimize swelling, and protect your repair.
You will be able to use your arm for tasks at the waist such as typing and cutting food. However, you will likely need assistance around the house.
You will wear your sling except for prescribed exercises.
Driving will not be permitted while wearing your sling or on narcotic pain medications.
Your first post-operative visit will be scheduled in the office during this time.
Weeks 3-6
Depending on your surgery, sling weaning may start between 3-6 weeks.
Continue with basic shoulder exercises.
Gradually reduce or eliminate the use of any narcotic pain medication prescribed after surgery.
Typically, you’ll have your second post-op visit scheduled in the office.
Week 6-8
Your sling can be removed.
It may be necessary to gradually wean your way out of the sling. Start by keeping your sling off while at home, Then progress to having it off in public.
Avoid heavy lifting during this phase of recovery.
Week 8-12
Patients can start to strengthen their shoulder by increasing their activities.
Activity can be increased as pain and strength allow.
Most patients do not attend formal physical therapy.
Week 12 and beyond
Most patients are working on functional activities in therapy or have discontinued them as they have reached their goals.
By six months after surgery, most patients will reach 80-90% of their final improvements.