Joint replacement can help relieve pain and enable you to live a fuller, more active life. If you and your orthopedic surgeon have decided that you are a good candidate for shoulder joint replacement, you are in good company. Over 50,000 people in the U.S. have shoulder replacement surgery each year.
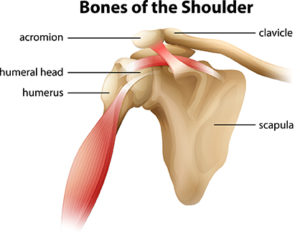
Shoulder anatomy
The shoulder joint is described as a ball and socket joint, which allows the shoulder to provide the wide range of motion required to perform many athletic activities, such as throwing, swimming, serving a tennis ball, and functional movement in many directions.
The “ball” component is made up of the head of the upper arm bone (humerus). The “socket” component, called the glenoid, is made up of the outer portion of the shoulder blade (scapula). The third bone is the collarbone (clavicle). The labrum is a rim of cartilage on the socket that helps stabilize the joint.
The stability of the shoulder joint mainly depends on the capsule, a strong envelope tissue surrounding the joint, ligaments connecting bones in the shoulder joint, tendons that attach muscles to bones, and the muscles themselves which initiate and control the position and activity of the joint. Also contributing to stability of the shoulder is the rotator cuff. The cuff formed of tendons attaches to the humerus and their four major muscles, which drape over the shoulder joint. The large muscles, which attach to the shoulder blade play a significant role in the normal function of the shoulder.
Causes and risk factors
Shoulder injuries Shoulder injuries can result from genetic factors, from overuse activities, or from a single traumatic injury. Many repetitive sporting activities that use the arm overhead, such as tennis, swimming, and baseball can result in injury to the capsule, ligaments, and muscles that surround the shoulder joint. Lifting weights too frequently or incorrectly can also lead to a shoulder injury. Immediate effects of these injuries can lead to pain, swelling, and instability of the shoulder.
Depending on the severity of the injury, the function of the injured arm can often be greatly compromised. Unfortunately, some structures of the shoulder joint do not readily heal themselves. Even with treatment, such as physical therapy, some of the symptoms or limitations may remain. Therefore, without surgical intervention, many individuals are unable to participate in their desired sports or functional activities at the pre-injury level.
Osteoarthritis This is an age-related “wear and tear” type of arthritis and a common reason that people have shoulder replacement surgery. The cartilage that cushions the bones wears away and the bones then rub against one another. Over time, the shoulder joint slowly becomes stiff and painful. In order to improve the function of the shoulder and restore motion, replacing the surfaces of the shoulder joint can be the most effective treatment to improve function and relieve pain. This can be accomplished by performing a shoulder replacement, which is also known as shoulder arthroplasty.
Surgery
The most common types of surgery are total shoulder replacement and reverse total shoulder replacement. In general, total shoulder replacement consists of putting new surfaces on the socket and humeral head. Reverse total shoulder replacement also allows for replacement of both surfaces, but does not rely on a functioning rotator cuff for motion or stability of the joint replacement. The decision to have shoulder replacement surgery, and which type, should be a collaborative one between you, your family, your primary care physician, and your orthopedic surgeon.
After surgery
Most patients are discharged home on the day of surgery unless medical issues dictate otherwise. You will be instructed how to put on and take off the sling or shoulder immobilizer and when to use it. Watch this video to learn more:
Cryotherapy, the use of cold to treat your shoulder surgery, is important to help decrease pain and reduce swelling and inflammation. You will be provided with a cold therapy unit to take home with you. Begin using it as soon as possible after you arrive home and continue using it for at least 5-7 days, during the day and night.
Your care team will provide you with prescriptions for pain medication, let you know how long to keep the dressing on, and detailed information on what to do after surgery for optimal recovery.
Recovery timeline
While not true for all patients, many will follow a similar plan during their recovery from surgery. In order to give you a sense of what is common following many shoulder surgeries we have outlined a normal post-operative timeline.
Weeks 1-2
You will work to get your pain under control, minimize swelling, and protect your repair.
You will be able to use your arm for tasks at the waist such as typing and cutting food. However, you will likely need assistance around the house.
You will wear your sling except for prescribed exercises.
Driving will not be permitted while wearing your sling or on narcotic pain medications.
Your first post-operative visit will be scheduled in the office during this time.
Weeks 3-6
Depending on your surgery, sling weaning may start between 3-6 weeks.
Continue with basic shoulder exercises.
Gradually reduce or eliminate the use of any narcotic pain medication prescribed after surgery.
Typically, you’ll have your second post-op visit scheduled in the office.
Week 6-8
Your sling can be removed.
It may be necessary to gradually wean your way out of the sling. Start by keeping your sling off while at home, Then progress to having it off in public.
Avoid heavy lifting during this phase of recovery.
Week 8-12
Patients can start to strengthen their shoulder by increasing their activities.
Activity can be increased as pain and strength allow.
Most patients do not attend formal physical therapy.
Week 12 and beyond
Most patients are working on functional activities in therapy or have discontinued them as they have reached their goals.
By six months after surgery, most patients will reach 80-90% of their final improvements.