Dr. Robert Sawin, retired pediatric surgeon, joined the St. Charles Health System Board of Directors in January 2026 – bringing more than three decades of experience as a health care provider, hospital system leader and medical school faculty member to his role on the board.
Sawin holds a Bachelor of Arts degree from Colgate University, a master’s degree in preventive medicine and environmental health from the University of Iowa and a medical degree from University of Pittsburgh. He completed his residency at Brigham and Women’s Hospital at Harvard Medical School and his fellowship at the University of Washington and Seattle Children’s Hospital.
Most of his career was spent at Seattle Children’s Hospital where he began practicing as a pediatric surgeon in 1987. He held a variety of leadership roles and also served as faculty for the University of Washington Medical School. In a volunteer capacity, he served on the Board of Directors and the Advisory Board for First Place, a school for houseless children and families in transition, for 16 years.
After retiring in 2020, Sawin relocated to Central Oregon where he and his wife have had a home since 2009.
Reason for Service: “St. Charles is unquestionably the most important institution in Central Oregon. A thriving health care system is an essential element of high-quality living in our region. As both a patient and a committed community member, I want to help assure its continued success and value for our region in any way that I can.”
St. Charles is transforming cardiology care for patients in Central Oregon, thanks to newly opened and updated electrophysiology (EP) labs and a cardiac catheterization (cath) lab at St. Charles Bend. These updates, funded with a $1.5 million investment from St. Charles Foundation, allow physicians to perform more advanced procedures and improve quality of life for more cardiac patients.
“Thanks to these updates, we can treat more patients and offer more state-of-the art services, allowing more cardiac patients to keep their care close to home,” said Lesley Jones Larson, Cardiac Service Line Administrator at St. Charles.
According to Larson, thanks to the new labs, the number of electrophysiology procedures performed has increased 27% from last year. Electrophysiology is a form of cardiology focusing on the heart’s electrical system that treats irregular heart rhythms. One advancement the team is particularly excited about is the ability to perform Pulse Field Ablations (PFAs).
“This is a minimally invasive treatment for patients who are experiencing atrial fibrillation (AFib). It uses non-thermal electric pulses to selectively destroy heart tissue. This is a significant advantage over older thermal ablation energies, as there is improved recovery and significantly lower risk to injuring structures surrounding the heart,” said Dr. Chris Lewis, cardiac electrophysiologist with St. Charles. “Ultimately, this allows us to perform safer procedures and offer atrial fibrillation ablation treatments to a larger group of patients.”
More than 285 patients have received a PFA in the new electrophysiology labs – a procedure patients used to travel out of the area to receive.
“The investment in this cardiology technology marks one of the largest projects funded by St. Charles Foundation in 2025. This effort means a great deal to our donors, as it allows St. Charles to be an early adopter of technology that is helping transform cardiac care for Central Oregonians,” said Jenny O’Bryan, executive director of St. Charles Foundation.
This spring more than 2,000 third graders throughout Central Oregon will learn about brain injury prevention and helmet safety through the Train Your Brain program taught by St. Charles athletic trainers. This program provides interactive assemblies and free multi-sport helmets to local elementary students across the region.
“Helmet safety is a simple yet crucial way to prevent serious head injuries in children,” said Stuart Schmidt, Athletic Training program manager at St. Charles. “With the Train Your Brain program, we create a fun, interactive experience that helps students develop lifelong safety habits and empowers them to protect their brains while staying active.”
For 16 years, the Train Your Brain program has distributed more than 1,000 free helmets for local students every year, ensuring kids have proper head protection for activities such as bicycling, skateboarding, rollerblading and scooter riding. The 2026 program, which is funded by St. Charles Foundation, begins in late March, just in time to prepare students for a safe and active summer. The presentations include interactive demonstrations on injury prevention, helmet safety, proper fitting and care. A highlight of the assembly is the melon drop, which is a dramatic demonstration that emphasizes the importance of wearing a helmet. Following the presentation, St. Charles caregivers and volunteers will properly fit free helmets for every student who needs one.
“We also want to thank our school districts for recognizing the significance of this safety initiative and to our partners, First Interstate Bank and the Redmond and Sisters Kiwanis clubs, for making it possible to provide free helmets to every third grader in Central Oregon who needs one,” said Schmidt.
To learn more about Train Your Brain and our athletic trainers, visit our webpage.
If you visit St. Charles Cancer Center in Bend, you may notice a bright pink wagon. Known as the Wig Wagon, this colorful cart is filled with wigs in all kinds of fun styles and colors, all offered at no cost to qualified patients thanks to support from Sara’s Project through St. Charles Foundation.
For many patients, hair loss is one of the more emotional parts of treatment, often affecting their confidence and sense of identity, according to Linda Robson, a social services associate with St. Charles. That's why Robson and Nurse Navigator Sadie Robinson started the Wig Wagon program — they saw firsthand the need for patients to have access to wigs to offer a sense of comfort during a difficult time.
“When a patient finds a wig they like, they are visibly lighter,” Robson said. “They’ll say, ‘This feels like me,’ and you can see the relief in their whole body.”
Since the Wig Wagon began in 2023, the program has provided more than 150 qualified patients with wigs, helping them feel like themselves again.
St. Charles Cancer Care is transitioning to a new name that better reflects the quality and breadth of services provided.
Today, I’d like to introduce the St. Charles Cancer Institute.
To be clear, the buildings (or physical spaces) where we treat patients will continue to be called St. Charles Cancer Centers. The St. Charles Cancer Institute is an umbrella name that encompasses the care provided within our multiple sites, along with our academic and research initiatives, multi-specialty collaboration, patient navigation, integrative therapies, genetics program, screening services, support services and so much more.
So, what does it mean to be a cancer institute?
First of all, it’s a designation our team has been working toward for many years. Dr. Linyee Chang, St. Charles Cancer Institute’s medical director, has spent decades recruiting and building a team of physicians and providers trained at some of the top cancer programs in the nation. That effort led us to the highly specialized team we have today, with oncologists who are laser-focused on a variety of cancers, including breast, gastrointestinal, malignant hematology (lymphoma, multiple myeloma), genitourinary, gynecologic, head and neck. This kind of specialization in particular cancers is the foundation of our ability to deliver institute-level care.
And, for more than 20 years, our team has meticulously followed National Comprehensive Cancer Network guidelines to ensure patients receive the agreed upon, best standard of care. Thanks to their track record, we launched an innovative pilot program with one health insurer in 2024 that provides most patients with instant authorization for their cancer treatment to begin.
Most recently, the cancer team has added new capabilities in terms of academic and research programs that elevate all the services provided within the Cancer Institute umbrella. Through a new AI-powered tool, patients can be screened and matched against an ever-expanding number of clinical trials happening nationwide. Knowing if your particular type of cancer can be treated through the latest and most innovative clinical trial programs – but still managed right here in Central Oregon – is an incredible benefit to our patients.
At St. Charles, our commitment is to deliver cancer care at the highest level, with the Cancer Institute overseeing all aspects of cancer care in our region, from standardization of seamless delivery to assurance of the highest quality of care achievable.
You’ll hear more about all the above in the coming months, but in the meantime, we are celebrating the good work that our cancer teams do every day, including the incredible effort that has gone into building the new St. Charles Cancer Center in Redmond. This beautiful facility will open next month and will have the capacity to serve up to 300 patients each day. For those patients dealing with a cancer diagnosis and treatment who live in our northern region, I hope that knowing you can receive care even a little bit closer to home will provide peace and healing.
I’d love to invite all of you to check out the new space at our ribbon cutting event at 4 p.m. April 16. This community celebration will give us a moment to not only reflect on the years of planning that went into the facility, but also to celebrate the impact it will have on patients, their families and our community in the decades ahead.
Earlier this month, Kathy Grandmason celebrated her 50th anniversary as a caregiver at St. Charles, where she works as a communications specialist in the Transfer Center.
It’s a position she is naturally qualified for.
“I’m kind of a chatty person — a Chatty Kathy,” she said with a laugh.
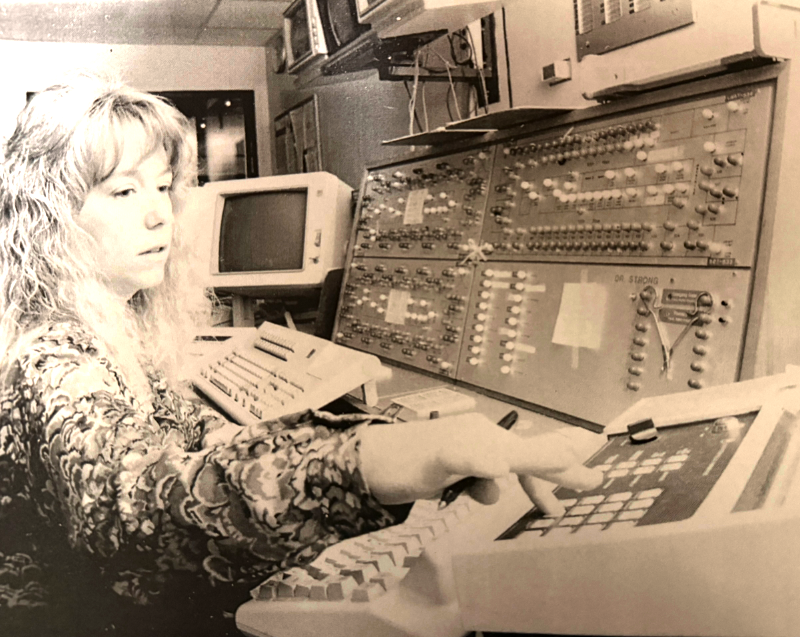
Grandmason has put those skills to work ever since she was hired to work the switchboard in 1976, about six months after St. Charles moved out of downtown Bend and into its then-new hospital on Neff Road.
Kathy Grandmason works the switchboard at St. Charles in the 1970s
“It was a wonderful place,” she said. “When you’d turn to go toward the hospital, it was all trees — all of these parking lots weren’t here. So you’d go down the little winding road and then, all of a sudden, you came upon this beautiful campus.”
Born in The Dalles, Grandmason moved to Bend when she was 5 years old, and she graduated from Bend High School in 1969. Shortly thereafter, she started taking classes at Central Oregon Community College, where she got a job working the switchboard, which at the time was the old “cord board” style that required operators to carefully crisscross cords across a grid of audio inputs.
“If something happened and you yanked the cord, they all might fall out. So it was a little stressful,” she said. “But I found I really liked it.”
After a few years, she met someone who had done the same job at St. Charles and enjoyed it. So she decided to apply for an opening.
“At first, I just needed a solid place to work,” Grandmason said. “And then it turned into talking to patients and helping patients and talking to people in the community and helping them get where they needed to go. And I loved it.”
Back then, St. Charles switchboard operators not only took incoming calls, they also responded when patients called to indicate they needed help; then, the operators would contact a nurse to let them know what the patients needed. They also handled nighttime admitting to the hospital, Grandmason said.
She remembers a time when she answered a call and could hear only noises in the room — no words. She messaged the nurse, who responded to find the patient choking.
“I felt like I was really helping. I had a job that really meant something, and that meant more to me than anything else,” she said. “I was helping people. I was a part of a team. I was really connected and helping the doctors and nurses. I felt like what I was doing was making a difference.”
Five decades later, Grandmason’s office has moved a few times, but she’s still making the same difference, said Elisa Ginabreda, supervisor of the Transfer Center.
“Her skill is her genuine kindness and the caring that she has. It’s who she is,” she said.
“She takes every call and really listens and tries to help people get to the right place,” Ginabreda continued. “She doesn’t rush a call if someone’s not understanding. She takes her time with every single person, and she does so in a manner where you can tell that she not only enjoys what she does, but she cares about the people that she's talking to.”
When asked what it takes to be successful in the job she has done for 50 years, Grandmason didn’t hesitate, and her answer echoed Ginabreda’s observation.
“I try to remember that when someone on the phone says something to me, it's their first time. It might be my 100th time hearing the same question, but it’s their first time asking it,” she said. “And people need to feel safe and feel encouraged that it’s OK to come here if they need to. So I need to be the front face for the hospital. I need to be the smile. I need to be welcoming, because we have a terrific team here.”
In addition to her sharp communication skills, Grandmason is an invaluable presence on that team, Ginabreda said.
“She brings a lot of insight and a lot of history to the office. There are things that only Kathy knows because she has been here,” she said. “I love when she’s working because she’s just a joy to be around. She elevates the day.”
Each year, thousands of teenagers die when their heart suddenly stops beating without warning, an event known as sudden cardiac arrest (SCA).
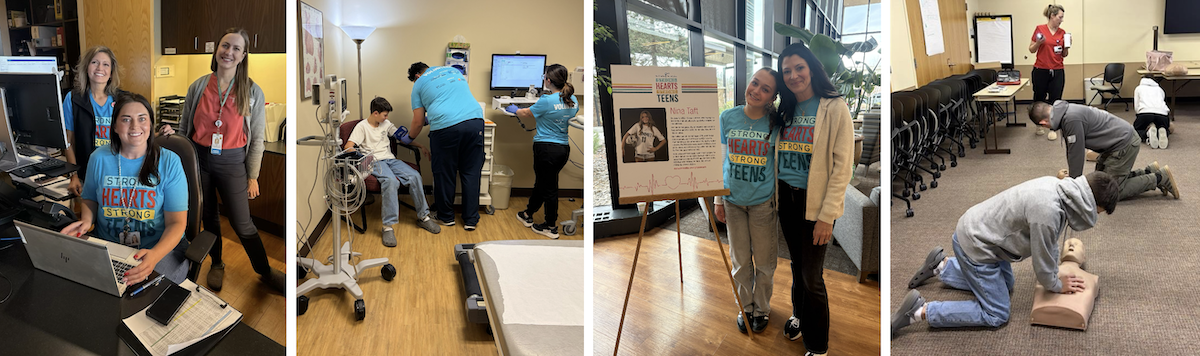
But SCA is preventable through awareness, education and direct intervention, and protecting our kids’ hearts is a responsibility we all share. That’s why St. Charles hosted a Strong Hearts, Strong Teens screening on Feb. 7 — because every teen deserves the opportunity to live a healthy, active life without this looming threat.
Led by St. Charles Cardiology in partnership with The Children’s Heart Center of Central Oregon, Strong Hearts, Strong Teens included a blood pressure check, EKG and limited echocardiogram plus AED and CPR training. This screening program is designed to detect four serious heart conditions that are not typically identified during a standard sports physical or well-child visit.
More than 100 students received free heart screenings at the event, which was made possible by community donations through St. Charles Foundation. Thank you to all the caregivers and volunteers who helped make Strong Hearts, Strong Teens a success!
St. Charles adds access to healthy, affordable foods as priority after report shows surge in need for Central Oregonians
Many Central Oregonians struggle to access affordable, healthy food and that need is increasing, according to results from the 2025 Community Health Needs Assessment recently produced by St. Charles Health System. The survey showed 24% of Central Oregonians said better access to affordable, healthy food is the factor that would most improve their overall quality of life, ranking higher than affordable housing (19%) or living-wage jobs (11%) and marking a significant increase from the 2022 report, when 15% of respondents picked affordable, healthy food as their top concern.
To address this growing need within the community, St. Charles Health System is adding improving access to affordable, healthy foods as a focus for its Community Benefit efforts. This means for the next three years, St. Charles will direct thousands in grant funding to community organizations that target access to affordable, healthy food as well as organizations that focus on fostering a sense of belonging and reducing loneliness (which has been the health system’s priority focus for the past three years and will continue through at least 2028).
Carlos Salcedo, manager of community partnerships for St. Charles, says the two priority areas make a lot of sense together. “As people, we know that food and community often go together, and sharing a meal can bring people together and help reduce loneliness. We are excited to fund projects that serve these important priorities and meet the needs we are seeing in our community.”
This priority, approved by the St. Charles Board of Directors in February, is also driving other efforts in the health system focused on access to healthy food. Kelly Ornberg, manager of clinical nutrition services for St. Charles, is launching a new program named Fuel in March aimed at helping patients with a malnutrition diagnosis. Ornberg says St. Charles dietitians work hard to provide healthy foods to these patients while in the hospital, but many patients with malnutrition struggle to secure affordable, healthy food when they return home.
“That’s one of the reasons these patients end up being readmitted to the hospital at a high rate. About 11 percent of patients with malnutrition end up being readmitted to the hospital within 30 days. Our goal is to change that trajectory,” said Ornberg. “With this new program, we are able to provide patients with 30 days’ worth of shelf-stable supplements for free, so they are able to get some basic nutrition when they return home.”
Ornberg says St. Charles outpatient dietitians follow up with these patients after discharge to connect them with community resources for longer-term support. With the initial funding, Ornberg expects they will be able to help about 500 patients across all four St. Charles hospitals.
“It feels so good to be able to do something to help bridge that gap,” said Ornberg.
Late last month, we kicked off an exciting project: The construction of our new Susan A. Ellings Inpatient Rehabilitation Unit at St. Charles’ Bend hospital.
Inpatient rehab is where our patients go to heal and recover from traumatic injuries and serious illnesses. It’s a busy place — caregivers there provided more than 11,000 therapy visits in 2025.
The current unit is small and outdated, but that doesn’t stop our team from doing incredible, restorative work. Constrained by the space, however, they can’t see enough people to meet what our region needs so hundreds must receive care far from home each year.
Which is why we’re building a new 23-bed unit with larger patient rooms, state-of-the-art technology and plenty of space for our patients, their families and our caregivers to work together toward healing, recovery and a restored sense of independence. It’s not a place people want to be, but if they need our services, then we want them here in Central Oregon.
You’ll hear more about the unit over the coming year. Today, though, I’d like to talk about the story — and the person — behind its name. St. Charles Foundation has been raising funds for this project for the past year, and a generous anonymous donor chose to name the unit in honor of Susan A. Ellings, who passed away in 2014.
Susan A. Ellings
“My mother was like sunshine in human form. Her love for everyone and everything was radiant,” said Julie Cox, Ellings’ daughter, a registered nurse who works in the St. Charles Clinical Education department.
“When I was growing up, she was always involved in the parent-teacher association or volunteering somewhere or working with the youth group at our church,” she continued. “Her passion for other people and her ability to see the light in people — regardless of their situation — is something that’s always at the forefront of my brain.”
The daughter of immigrants from Germany, Ellings was born in Chicago and moved to Beaverton in her early teens, Julie said. After college, she worked at Fred Meyer headquarters, where she met her husband Joe, and the two opened a signage and graphics business together, which they ran until Susan got sick, at which point Joe closed up shop to focus on taking care of his wife.
While reflecting on her mom, Julie cited an old story you may have heard:
An old man had a habit of early morning walks on the beach. One day, after a storm, he saw a human figure in the distance moving like a dancer. As he came closer he saw that it was a young woman and she was not dancing but was reaching down to the sand, picking up starfish and very gently throwing them into the ocean.
"Young lady," he asked, "Why are you throwing starfish into the ocean?"
"The sun is up, and the tide is going out, and if I do not throw them in they will die."
"But young lady, do you not realize that there are miles and miles of beach and starfish all along it? You cannot possibly make a difference."
The young woman listened politely, paused and then bent down, picked up another starfish and threw it into the sea, past the breaking waves, saying: "It made a difference for that one."
“That totally encompasses who my mom was,” Julie said.
When I hear that, I can’t help but think about the incredible care that happens every day in the inpatient rehab unit. No matter how big we build, our team won’t be able to help everyone who needs it. But for the people they are able to see, they make a life-changing difference.
I hope Susan Ellings would be proud to have her name on a place like that.